

Cryptophthalmos (Greek, Kryptos is “hidden”)

severe cryptophthalmos
A rare failure of lid differentiation
Skin over eye (no lids or palpebral fissure) that frequently blends in with the cornea which is usually malformed
Ankyloblepharon

Ankyloblepharon
Fusion of part or all lid margin: variant: Ankyloblepharon filiforme adnatum in which the lid margins are connected by fine strands.
Epiblepharon

Epiblepharon
A horizontal fold of skin adjacent to either the upper or lower lid Tolerated well by the cornea
More commonly the lower lid
Often spontaneously resolves in the initially years of life
Surgery only indicated for severe cases or those that persist or cause corneal irritation and tearing.
Congenital coloboma (greek "Koloboma" means defect)

Coloboma of right upper eyelid
Often well tolerated Involves primarily the upper lid
no keratopathy
Congenital entropion (also called epiblepharon)

Epiblepharon (lower eyelid entropion)
Usually involves the lower lid
Distal part of tarsus rotated inward
Lashes abrade the cornea causing keratopathy
Permanent corneal damage is uncommon

right upper eyelid tarsal kink
Child is born with the upper lid bent backwards often with a 180 degree fold in the upper tarsal plate
Corneal exposure and rubbing by the bent edge can lead to in ulceration
"Well, the last time I had a picture taken I could hardly see my eyes because of the weight of heavy eyelid. Then I paid attention to how I was actually using my eyes and I really noticed when I was looking at anything especially the computer I was straining my forehead to see better. Since I have had it done I no longer have to lift the forehead and tilt my head to see. It is amazing! I love..." D. Rock 63 Yrs Old with Fat Droopy Eyes - Salt Lake City, UT
Distichiasis

An accessory row of lashes growing from the meibomion orifices or posteriorly.
The lashes are thinner, shorter, less pigmented and often well tolerated.

Distichiasis. Lashes growing out of the meibomion orifices.
Euryblepharon
Euryblepharon is defined by Duke-Elder (I964) as a symmetrical enlargement of the palpebral aperture occurring as a primary abnormality associated with large eyelids, and by Waardenburg, Franceschetti, and Klein (I96I) as bilaterally symmetrical large eyelids opening much wider than the normal, especially at the lateral but also at the medial end. Waardenburg and others (I96I) also stated that the presence of the condition at birth and the absence of ,any primary ocular abnormality distinguished euryblepharon from the secondary enlargement of the palpebral aperture which may accompany a variety of ocular abnormalities.
The condition was first described by Desmarres (I854), and subsequent reports in the German and Dutch literature by Schreiber (I924), Lindberg (I928), Seefelder (1930), and Weve (1936) are quoted by Duke-Elder (I964).
Epicanthus
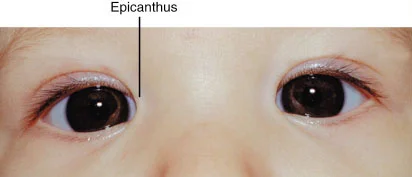
Crescentic fold of skin running vertically between the lids and overlying the inner canthus. There are three types:
Inversus: If the fold is most prominent in the lower eyelid
Tarsalis: (Most people) The fold is most prominent in the upper eyelid
Palpebralis: If the fold is equally distributed in the upper and lower eyelids.
Telecanthus (Greek “tele” meaning far and Latin “canthus” meaning corner of the eye: an example of the use of both, Greek and Latin in one medical word).

Normal interpupillary distance but wide intercanthal distance i.e. Waardenburg's syndrome
not: Hypertelorism, which indicates increased distance between the bony orbits.

"I had a excellent eye lift done by Dr. Patel. He knows what he is doing and is very pleasant. Dr.Patel was easy to get an appointment and he works with you. The office staff was very pleasant and made you feel calm." D. Gull Highly recommended for eye lift surgery - Salt Lake City, UT
Blepharophimosis

Vertically and horizontally shortened Syndrome palpebral fissures
Epicanthus inversus
Telecanthus
When should the Ptosis be repaired?
Frontalis slings are usually done early in life
Repairing telecanthus and epicanthus which may possibly improve with age is delayed
Lipodermoid

Lipodermoids are epibulbar, developmental growths of normal adipose in an abnormal site, ie. near the lacrimal gland and extending between the superior rectus and lateral rectus muscles posteriorly.
Differentiation of benign lipodermoids from non-benign lesions is essential.
When other ocular anomalies or systemic conditions are found in conjunction with lipodermoids then Goldenhar-Gorlin syndrome must be considered.
Congenital obital conditions
In the human embryo, the eyes are formed by a delicate and complex process. Problems in this process can lead to congenital (present at birth) eye malformations. These conditions are relatively rare, occurring in approximately five per 10,000 live births. Children with these problems need the kind of specialized experience found within our team at Primary Children’s Hospital in Salt Lake City.
What are congenital/developmental anomalies affecting the eye and orbit?
The human eye forms through a complex program during embryonic development. Problems in this developmental process can lead to congenital eye malformations, such as anophthalmia (no eye), microphthalmia (small eye), coloboma (failure of the optic fissure to close), aniridia (absent or partial iris), and optic nerve hypoplasia (underdeveloped optic nerve).
Conginital nasolacrimal duct obstruction
Overview, Signs and Symptoms of an Obstruction
The lacrimal gland produces tears which enter into the "duct"
that drain the tears from the eye into the nose. The most common symptoms are If one has a plugged up "tear duct," not only will tears spill over the eyelids and
run down the face, but the stagnant tears within the system can become infected.
excess tearing (tears might possibly run down the face) and
mucous discharge
This might possibly lead to recurrent red eyes and infections.
The excessive tearing can also produce secondary skin changes on the lower eyelids.
Congenital Nasolacrimal Duct Obstruction
Nasolacrimal Duct Obstruction (NLDO) is very common in infants.
Children are often born with an obstruction within the "tear duct." In fact, 6% of all children are born before their tear ducts are open.
The stagnant tears within the "tear duct" often become infected causing pus (heavy matter) to collect between the eyelids.
Antibiotics might possibly help some of the symptoms, BUT this is not cure for the blockage
Such obstructions might possibly resolve spontaneously within the initially few months of life. In fact, 95% of these children will show resolution before their initially birthday. If it does not resolve surgery might possibly be necessary.
Blockage presents in one of four ways:
simple obstruction
congenital fistula (as seen in the photo)
acute dacryocystitis
congenital dacryocele or mucocele

Dacryocystocele or dacryocele
Location of blockage and anatomy







The very end of this duct is the most common place for blockage to occur. This site is called the valve of Hasner at the distal nasolacrimal duct and might possibly represent failure of canalization of the epithelial cells that form the duct.
Medical Treatment of Congenital Obstructions
Many of these do open on their own given time.
Massaging from the tear sac in the might possibly help create a pressure wave that can open the blockage.
Surgical Treatments
Simple probing is followed by serial dilatation and intubation with a stent. In stubborn cases, balloon dilatation and stenting is needed. In older children, a dacryocystorhinostomy may be necessary.